Endourology Treatments & Diagnosis
Minimally Invasive Endourology
Endoscopic diagnosis and treatment for BPH, kidney stones, and other urinary tract conditions, including PCNL and paediatric endourology.
Treatments & Diagnosis for Endourology
Endourology uses endoscopes, thin instruments passed through the body's natural passages, to diagnose and treat urinary tract conditions without the larger incisions traditional surgery requires. It covers everything from an enlarged prostate to kidney stones.
Problems Treated
Benign Prostatic Hypertrophy (BPH)
Benign Prostatic Hypertrophy (BPH)
The prostate is a small gland unique to men, sitting in front of the rectum and surrounding part of the urethra, the tube urine passes through. It produces part of the fluid that carries and nourishes sperm, and continues to function into old age.
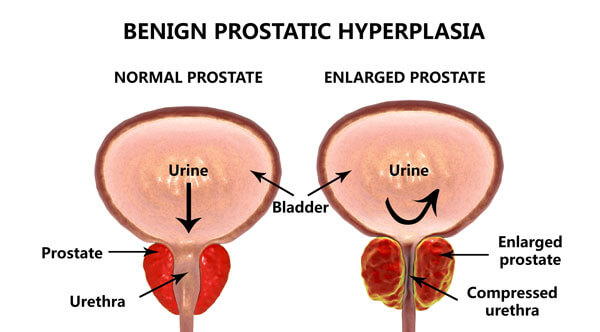
Benign Prostatic Hypertrophy (BPH) is non-cancerous enlargement of the prostate, common in older men. The prostate grows during puberty and, for many men, keeps growing gradually after around age 45 due to hormonal changes. The enlargement itself isn't dangerous, but as it presses on the urethra, it can disrupt normal urine flow.
BPH becomes more common with age, affecting roughly 4 in 10 men over 55 and around 7 in 10 men in their 70s. Symptoms may include:
- Frequent urination, especially at night
- A sudden, uncontrollable urge to urinate
- A weak urine stream
- A feeling of incomplete bladder emptying
- Difficulty starting urination
- Urinary incontinence
- Urine blockage
- Blood in urine
- Urinary infections
BPH Diagnosis Methods
Diagnosing BPH usually involves a combination of the following:
Medical History: A review of your past and current health conditions and medications.
Digital Rectal Examination: Examining the prostate through the rectum to assess its size and firmness.
Urine Testing: A urine sample checked for signs of infection or other issues.
Urine Flow Test: A flowmeter measures the strength of your urine stream to detect possible blockages.
- Ultrasound Scan: Images of the prostate to assess its size and any effect on the kidneys and bladder.
- Urodynamic Study: Used in some cases to measure bladder pressure directly.
- Post-Voiding Residual Measurement: Checks how much urine remains in the bladder after urination, via catheter or ultrasound.
- Cystoscopy: A thin scope used to directly examine the urinary tract for blockages or abnormalities.
Treatment for Benign Prostatic Hypertrophy (BPH)
Treatment for BPH depends on how severe your symptoms are, and your urologist will walk you through which option fits your case:
Medical Management
Usually appropriate for mild symptoms with minimal obstruction. These medications are typically taken long-term and offer meaningful, though not complete, symptom relief (around 20-30% improvement). Options include:
- 5 alpha-reductase inhibitors: Gradually reduce prostate size over time, though not suitable for every type of enlargement.
- Alpha-blockers: Relax the prostate muscles for faster symptom relief, without addressing the underlying enlargement.
Surgical Management
Surgery is generally the most effective way to relieve BPH symptoms long-term. The standard procedure is TURP (Transurethral Resection of the Prostate), which removes the innermost prostate tissue to relieve the obstruction:
- TURP (Transurethral Resection): An endoscope is passed through the urethra to remove prostate tissue, widening the passage and easing pressure on the urethra. It's minimally invasive and typically takes 1 to 2 hours.
For larger prostates (over 100 grams), HOLEP (Holmium Laser Enucleation of the Prostate) is generally the better option.
Post-Operative Effects
TURP relieves symptoms effectively, but it does carry known side effects worth discussing beforehand:
- Retrograde ejaculation, where semen enters the bladder instead of exiting the body, occurs in up to around 50% of patients and is often permanent.
- Urinary incontinence is uncommon but can occur, either with straining or continuously.
- A small percentage (around 2%) may experience temporary or permanent erectile dysfunction.
Tissue removed during surgery is routinely checked for malignancy, though BPH itself is benign. Treating BPH does not prevent prostate cancer, which develops in a different part of the gland, so annual check-ups are still recommended after surgery.
When to Seek Treatment
Not every enlarged prostate needs treatment; mild symptoms may simply be monitored. But if symptoms are significant, or tests show real impact on the urinary tract, it's worth acting sooner rather than waiting.
Percutaneous Nephrolithotomy (PCNL)
Percutaneous Nephrolithotomy (PCNL) is a minimally invasive procedure for removing kidney stones or stones in the upper ureter, generally offering faster recovery and a high success rate compared to open surgery.
Illustration of How PCNL is Performed
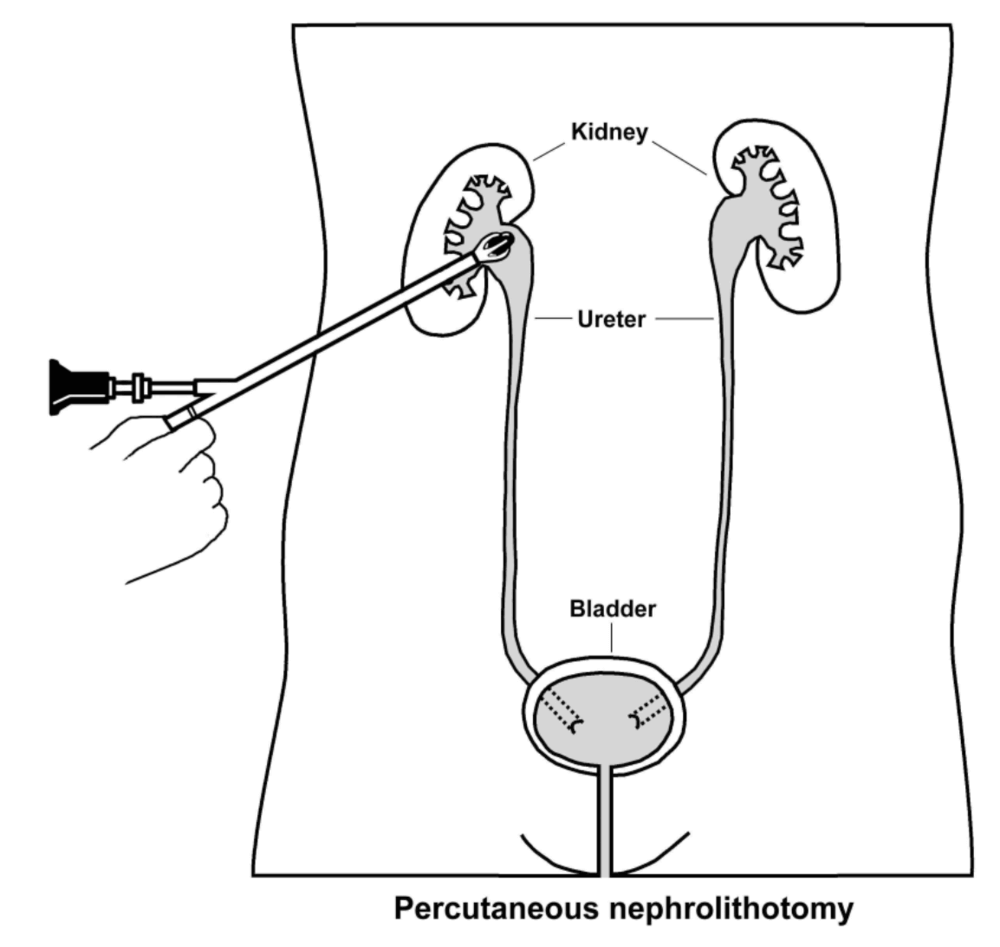
The procedure uses a small incision, typically 1 cm or less, in the flank. A guide wire is passed into the kidney under x-ray guidance, then a nephroscope is used to locate and remove the stone, fragmenting larger stones as needed. A drainage tube usually stays in place for 1-2 days afterward to support healing.
Compared to ESWL (shockwave therapy) or ureteroscopy, PCNL can often clear stones in a single session, which is why it tends to mean a shorter overall recovery, typically a hospital stay of 3-4 days.
It's generally recommended for kidney stones larger than 2 cm, upper ureteric stones larger than 1 cm, or lower pole kidney stones that don't respond well to other methods, and it's often used after medical therapy or ESWL hasn't worked.
PCNL is usually performed under general anesthesia with hospital admission, though intravenous sedation, regional, or local anesthesia may be used in certain cases.
Stone clearance success rates range from about 90% to 95%, depending on the stone's size, number, and location. A second procedure is sometimes needed for complete clearance.
Patients typically stay in hospital 2-3 days post-operatively, with x-rays or ultrasound used to check for remaining fragments. If fragments are found, further treatment such as another nephroscope session or ESWL may follow.
PCNL is generally safe, but like any surgery it carries some risk, including bleeding (around 1%) and infection. Some patients experience prolonged urine leakage from the flank, which may need a ureteric stent, and fever after the procedure may call for adjusted antibiotics.
Paediatric Endoscopes
We're equipped with a full range of paediatric endoscopes for both upper and lower urinary tract procedures, including cystoscopy, resectoscope, urethrotome, ureteroscope, and nephroscope, covering a wide range of paediatric urology conditions.